
Call Light Access for Residents with ALS: A Stage-by-Stage Plan for Care Teams
ALS changes what a resident can do, and it changes on a timeline the care team cannot fully predict. The nurse call button that worked in April may not work in July. The touch pad that worked yesterday may fail tomorrow after a bad night's sleep. This guide is for occupational therapists, DONs, speech-language pathologists, and family advocates who need to plan call access for a resident with ALS in a way that adapts as function declines, including in the late stage when both hand function and natural speech are gone.
Call access for a resident with ALS is not a single decision. It is a plan that has to evolve alongside the disease. The standard nurse call button assumes reach, grip, and press. ALS removes those capabilities in a sequence that is different for every person. A workable plan reassesses what the resident can reliably do every few months, then matches the call-access method to the current stage. When the resident's own voice is no longer reliable, voice-activated options do not automatically disappear. If the resident already uses an eye-gaze or AAC device, that device can carry the voice.
How ALS changes what a resident can do
Call-access methods should adapt as ALS progresses. The right option depends on what the resident can reliably do at each stage.
ALS affects motor neurons, which means it takes away the physical actions the standard call button depends on. The sequence and pace vary. Two residents with the same diagnosis rarely progress the same way.
Roughly, the picture looks like this:
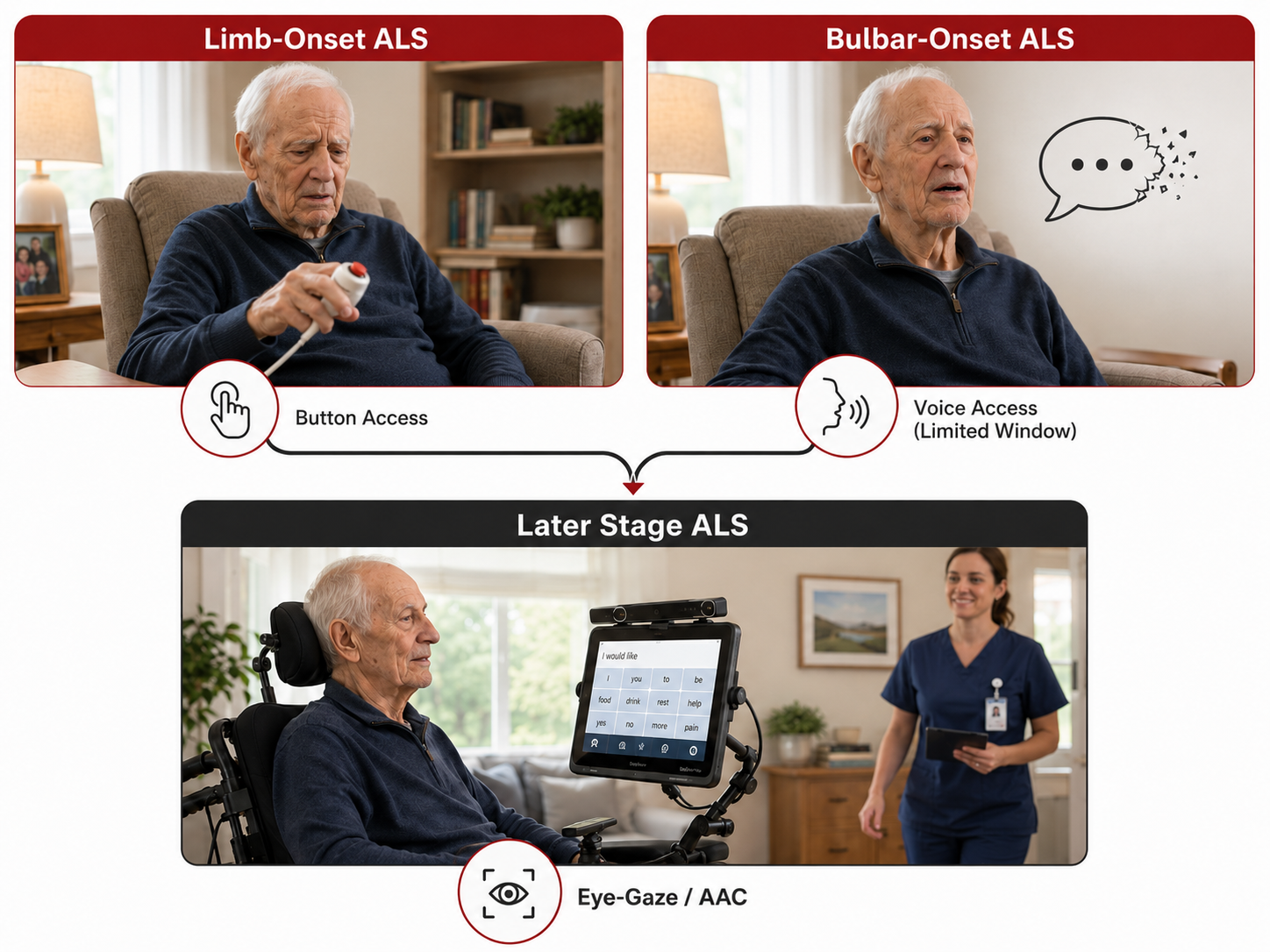
- Limb-onset ALS usually starts in the hands, arms, or legs. Hand and arm weakness are often the earliest disabling symptoms. Grip weakens, fine motor control declines, and the resident may still be able to press a button with the palm or thumb but not consistently. Natural speech is typically preserved longer.
- Bulbar-onset ALS affects speech and swallowing early, sometimes before limb function is significantly impaired. About 30% of people with ALS have bulbar onset, according to the ALS Association. For these residents, natural-voice-based call systems have a narrower window of usefulness or may not be appropriate at the outset.
- Later stages for either onset type typically involve loss of hand function, loss of head control, and often loss of natural speech. Many residents at this stage use eye-gaze or other AAC (augmentative and alternative communication) devices to speak on their behalf.
Key point: Two residents with the same ALS diagnosis can have very different call-access needs. Start with what the resident can reliably do today, not with the diagnosis.
The clinical reality behind call-access planning is that whatever works today has an expiration date. Peer-reviewed research on assistive technology use in ALS consistently finds that abandonment is high when a device is not matched to the current stage of function. Devices introduced too early are rejected. Devices introduced too late fail because the resident can no longer learn or activate them. Timing is not a nice-to-have. It is central to whether the plan works.
Why the standard nurse call button stops working
The standard nurse call button assumes six things about the resident: they can reach it, grip it, press it, locate it visually or by memory, sustain the press long enough to register, and (in some setups) call out to draw attention.
ALS chips away at those capabilities in different orders. A resident may lose grip strength months before they lose reach. They may retain the ability to press but lose the ability to locate the button if it slips into the sheets. Fatigue matters too. The same resident who could press the button in the morning may not be able to press it after physical therapy or a long visit.
When the standard button starts to fail intermittently, the plan often reacts rather than adapts. Staff move the button closer. Family members reposition it. Someone finds a lightweight touch pad. These are reasonable short-term responses, but they are not a plan. A plan looks at what the resident can reliably do at this stage, what they will likely lose next, and what the next call-access method should be.
The call-access options and where they fit
There is no single right device for a resident with ALS. There is a set of options, each with a stage where it fits and a stage where it stops fitting. Here is how the common options map to ALS progression.
Modified push buttons and lightweight touch pads
These reduce the force required to activate the call. They fit early in disease progression when grip is weakening but the resident can still press with a finger, palm, or side of the hand. They are simple to introduce and require no new infrastructure.
They stop fitting when the resident can no longer sustain contact with the surface, or when hand positioning becomes unreliable. A pad that requires deliberate contact will not work for a resident whose hand rests inconsistently on the surface.
Sip-and-puff systems
Sip-and-puff activates a call by drawing air in or blowing air out through a mouthpiece. It fits residents with limited hand function who still have strong, reliable breath control.
For ALS, this option has a specific limitation: bulbar symptoms and reduced respiratory function can make sip-and-puff unreliable or unusable. It may work for limb-onset ALS at a certain stage. It is often not a good fit for bulbar-onset ALS, and it stops fitting for anyone as respiratory function declines.
Soft switches, proximity switches, and head-activated switches
These require less strength than a button and can be positioned near a hand, cheek, or head. They fit residents who retain some reliable movement in a specific body part, even if that movement is small.
They stop fitting when the reliable movement itself is lost. A head switch that works when head control is present will fail when head control declines.
Voice-activated call systems (natural speech)
Voice activation lets the resident say a phrase and trigger the existing nurse call system. It fits residents who can still speak clearly and consistently enough for the device to recognize the phrase.
For ALS, the window depends on onset type. Limb-onset residents often have a long window where their voice is reliable and their hands are not. Bulbar-onset residents may have a shorter window or none at all. Fatigue affects speech clarity, so an assessment done in the morning may not reflect what the resident sounds like in the evening.
A resident with ALS in this window can be a good fit for a voice-activated nurse call accessory such as Will-Call, which listens for the phrase "I need help" and activates the existing nurse call system through the same jack a standard button would use. This is one of the situations Will-Call was designed for, and it is illustrated in a story from Maple Lawn Nursing & Rehab, which used Will-Call for a resident with advanced ALS whose hand function had declined past the point of button use.
Fit criteria to check before deciding voice activation is the right next step:
- Can the resident speak the activation phrase clearly across different times of day and levels of fatigue?
- Is the resident cognitively able to retain and use a specific phrase?
- Does the room have a compatible existing nurse call jack?
- Can the microphone be positioned close enough to reliably capture the resident's voice?
Voice activation with the resident's natural voice stops fitting when speech becomes unreliable. In the past, that has usually been treated as the end of the voice-activation option. It does not have to be.
AAC and eye-gaze paired with voice-activated call
This is the option most call-access planning for ALS misses. If the resident already uses an eye-gaze or other AAC device to communicate, that device can speak the activation phrase on their behalf. The nurse call system does not need to hear the resident's natural voice. It needs to hear the phrase.
"For most people, that combination, no reliable hand movement and no reliable voice, would seem to close the door on voice-activated call systems entirely."
— Will-Call customer story, resident with advanced ALS using an eye-gaze communication device
In the documented case of a resident with advanced ALS using an eye-gaze device, the care team configured Will-Call to listen for "I need help" spoken by the synthesized voice of the eye-gaze device. When the resident selected the phrase on her screen, the device spoke it, Will-Call recognized it, and the existing nurse call system activated. The alert behaved exactly like a standard button press for the staff. For the resident, it meant she could call for help using the same tool she already used every day to speak with her family.
This pairing has specific fit criteria:
- The resident is a reliable daily user of an AAC or eye-gaze device
- The device can be configured to speak the activation phrase clearly and consistently
- The microphone can be positioned to capture the AAC device's audio output
- The existing nurse call system is compatible with Will-Call
- The care team is willing to test the setup in the actual room before committing
Where those pieces are in place, this option can restore independent call access at a stage of disease where it is often assumed to be lost.
How to build a plan that adapts
The ALS Association's guidance on assistive technology is direct: communication and call systems must evolve with the person. AOTA practice guidance for progressive conditions says the same thing in different words, recommending ongoing functional assessment and decisions made with the expectation of change rather than as one-time recommendations.
A workable plan for a resident with ALS has three parts.
Reassess on a cadence, not a crisis
The Muscular Dystrophy Association recommends reassessing adaptive equipment every few months for residents with ALS. Not annually. Not when something breaks. Every few months, tied to visible changes in function.
At each reassessment, check the six capabilities against the current call-access method. If the resident can still activate reliably, keep the current method and note what to watch for. If activation is becoming inconsistent, plan the transition to the next option before the current one fails completely.
Introduce the next option before the current one fails
The research on assistive technology abandonment is clear that devices introduced too late fail because the resident can no longer learn them. If voice activation is likely to be the next step, introduce the activation phrase while the resident can still practice it reliably. If an AAC pairing is likely to be the step after that, get the AAC device configured and part of daily use before it becomes the only remaining option.
Match the option to the resident, not the diagnosis
The diagnosis informs the assessment. It does not determine the answer. Two residents with limb-onset ALS at the same stage may need different call-access methods based on cognition, room layout, existing communication tools, and personal preference. The plan is built around what the resident can reliably do and what they already use, not around what "ALS residents typically need."
When voice-activated options are not the right fit
Voice activation is not right for every resident with ALS. Bulbar-onset residents without an AAC device may not have a reliable voice at any stage of disease. Residents with significant cognitive changes may not be able to retain the activation phrase. Rooms without a compatible nurse call jack may need infrastructure changes before voice activation is possible.
In those situations, the plan should focus on the options that fit: reliable positioning of a switch the resident can still activate, staff rounding tied to specific times, and family or caregiver presence during high-risk windows. Voice activation should be considered when the pieces are in place, not forced when they are not.
FAQ
How does ALS affect a person's ability to use a call button?
ALS weakens the motor neurons that control voluntary movement, so the reach, grip, and press that a standard call button depends on become unreliable over time. The pace and sequence vary by person. Some residents lose grip first, others lose reach or the ability to sustain a press. Fatigue also affects reliability, so the same resident may be able to press the button in the morning and not later in the day.
What call button options exist for someone with ALS?
The main options are modified push buttons and touch pads, sip-and-puff systems, soft or head-activated switches, voice-activated nurse call accessories, and voice-activated systems paired with an AAC or eye-gaze device. Each option fits a specific stage of function. The right choice depends on what the resident can reliably do right now, not on the ALS diagnosis alone.
When should a family or facility switch from a button to a voice-activated call device?
When button activation becomes inconsistent, not when it stops working entirely. Waiting until the button fails completely often means introducing the new device at a stage where the resident has more difficulty learning and practicing the activation phrase. If voice activation is likely to be the next step, start the conversation while the resident can still reliably press the button occasionally.
Can a person with ALS use a voice-activated nurse call?
Yes, when they can speak the activation phrase clearly and consistently, when they can retain the phrase, and when the room has a compatible nurse call system. Voice activation is one option to consider based on those fit criteria. It is not a default answer for every resident with ALS.
What happens when someone with ALS loses their voice?
Natural-voice activation stops being reliable, but voice activation as a category does not necessarily end. If the resident uses an AAC or eye-gaze device, that device can be configured to speak the activation phrase, and a voice-activated call accessory can be set up to listen for the synthesized voice instead of the natural voice.
Can an eye-gaze or AAC device be used to call for help?
Yes, in the right setup. When the AAC device is part of the resident's daily use, when it can speak a specific activation phrase clearly, and when a voice-activated call accessory is positioned to hear that phrase, the AAC device becomes a pathway to the existing nurse call system. This has been documented with a resident in advanced ALS using an eye-gaze device paired with Will-Call.
Next step
If you are supporting a resident with ALS and their current call-access method is starting to fail, the most useful next step is a reassessment against the six capabilities and a conversation about what the next stage looks like. An occupational therapist or speech-language pathologist familiar with progressive conditions can help build the transition plan.
If you want to evaluate whether voice activation, alone or paired with an AAC device, fits a specific resident in a specific room, request a 30-day Test Drive so the setup can be tried in the actual environment before any purchase decision.